Treatment Summary
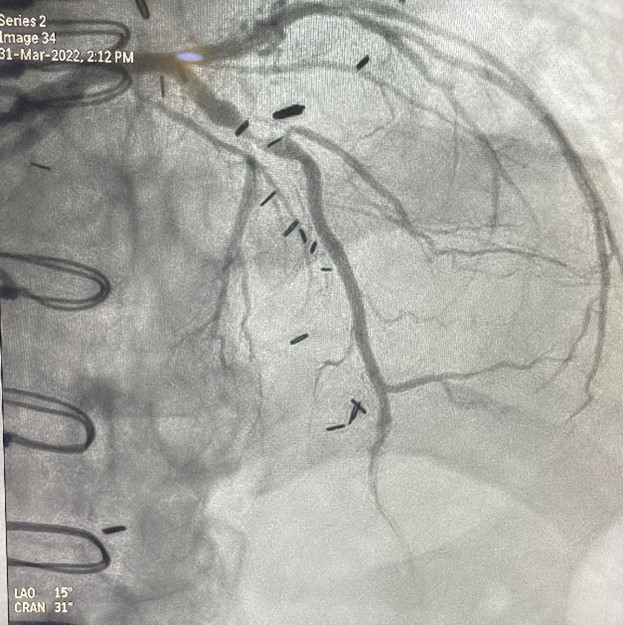
Access to the left anterior descending artery (LAD) was obtained with a right radial approach using a 7 Fr sheath. The Physician wired the vessel and advanced a microcatheter across the lesion, exchanging to the ViperWire Advance® with Flex Tip.
The Diamondback 360 Coronary Orbital Atherectomy System (OAS) was prepped and tested outside of the body before being inserted over the ViperWire Advance with Flex Tip. GlideAssist® mode was used to advance the catheter proximal to the mid LAD lesion. Treating this lesion antegrade, three orbital atherectomy (OA) passes were performed at low speed, the first for 30 seconds, the second for 29 seconds, and the third for 30 seconds, with equal rest periods between each pass. After OA was performed, the device was removed with GlideAssist. The microcatheter was then inserted over the ViperWire Advance with Flex Tip, to exchange back to the workhorse wire.
Post OA intravascular ultrasound (IVUS) found residual dense 360-degree calcium but no residual endoluminal nodular calcium. A Sapphire® NC 3.5 mm x 15 mm coronary dilation catheter was advanced and inflated in the mid LAD. Despite the endoluminal plaque modification, a residual balloon waist was noted requiring deeper calcium modification. Coronary Intravascular Lithotripsy (IVL) was then performed with a 3.5 mm x 12 mm for 80 pulses. A 3.5 mm x 28 mm stent was delivered and expanded, following with a Sapphire NC 3.5 mm x 15 mm and 4.0 mm balloons for post-dilation followed by IVUS.
The circumflex artery and obtuse marginal (OM) were treated using Sapphire NC 3.0 mm balloon. After IVUS, a 2.75 mm x 32 mm stent was delivered and expanded into the OM2. Post-dilation was performed using a Sapphire NC 3.0 mm balloon and a Sapphire NC 4.0 mm was inflated proximally.
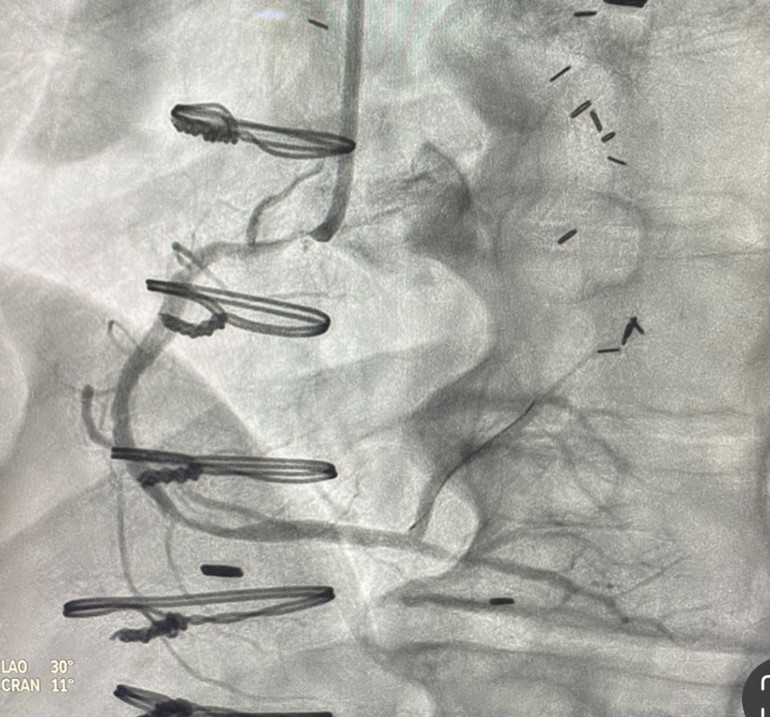
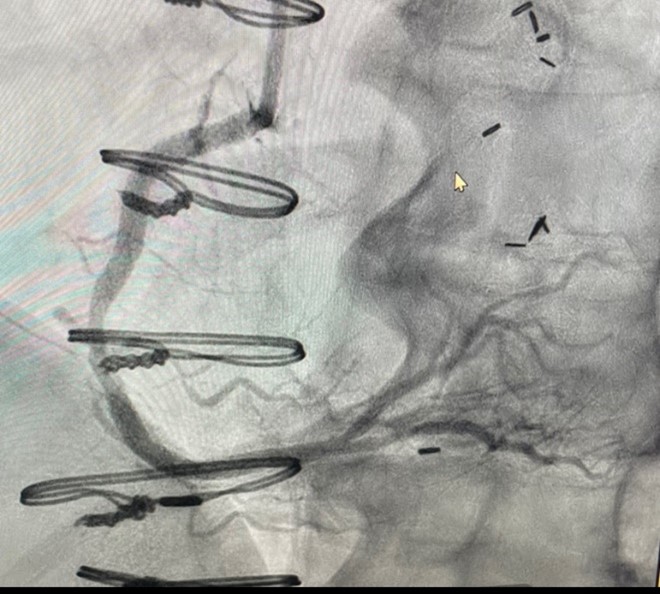
The ostial right coronary artery (RCA) stenosis was treated last and was accessed by the same right radial approach. The ViperWire Advance with Flex Tip was used to primary wire the artery. The Diamondback 360 Coronary OAS was inserted and advanced proximal to ostial lesion via GlideAssist. Due to the original of the ostial stenosis, the crown was advanced through the lesion via GlideAssist to treat the lesion in a retrograde fashion, starting with the crown distal to the lesion moving proximal. Three OA passes were performed at low speed, the first for 25 seconds, the second for 25 seconds, and the third for 30 seconds.
After the OA was performed in the RCA, the microcatheter was inserted over the ViperWire Advance with Flex Tip to exchange to workhorse wire. Following IVUS, a Sapphire NC 3.5 mm x 18 mm coronary dilation catheter was inflated, followed by two DES stents, 3.5 mm x 28 mm and 3.5 mm x 38 mm. Post-dilation with a Sapphire NC 3.5 mm x 15 mm, then 4.0 mm balloons were performed before final IVUS images and measurements obtained.
The total procedure time was 115 minutes.
Total fluoroscopy was 43 minutes, 1979 mGY. 275 mL of contrast dye utilized.